Bulbous Tip
One of the most common complaints heard at a rhinoplasty consult is ‘I hate the round ball at the end of my nose’. In medical terms this is described as a bulbous tip. The two main causes of the bulbous nasal tip is tip cartilage shape/support and skin thickness.
If the deformity is caused by robust nasal tip cartilages, the problem with the cartilage is often threefold:
- Too much vertical fullness of the lateral crura
- Strong convex lateral crural cartilages
- Vertically oriented lateral crural elements
These three lateral crural characteristics are addressed using the following techniques:
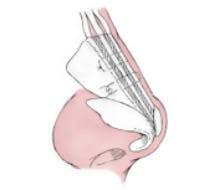
- Cephalic trim of the cartilages edges while leaving at least 6 mm of lateral crural width
- Underlay cartilage graft technique (ideally using straight septal cartilage that when secured to the undersurface of the lateral cartilage convexity results in straightening
- Lateral crural repositioning (by reorienting the lateral crura to more adequately support the sidewalls of the nose